Thank you for your interest in CCO content. As a guest, please complete the following information fields. These data help ensure our continued delivery of impactful education.
Become a member (or login)? Member benefits include accreditation certificates, downloadable slides, and decision support tools.

Associate Professor of Pharmacy Practice
Duquesne University Mylan School of Pharmacy
Pittsburgh, Pennsylvania
Jamie L. McConaha, PharmD, NCTTP, BCACP, CDCES, has no relevant conflicts of interest to report.
In this companion commentary to the live webinar “Moderate to Severe Atopic Dermatitis: Targeted Pathways and Strategies to Personalize Patient Care,” Jamie L. McConaha, PharmD, NCTTP, BCACP, CDCES, discusses the current understanding of the pathophysiology of atopic dermatitis (AD) and the ever-changing landscape of biologic treatment for AD.
New Paradigms in Pathophysiology of AD
Several factors contribute to the pathogenesis of AD, including both epidermal- and immune-based mechanisms (Figure 1). In the epidermal model, genetic epidermal barrier defects trigger abnormal keratinocyte aplasia such as mutations in the FLG gene encoding the filaggrin structural protein, which is one of the strongest genetic risk factors for AD. For patients with AD and FLG mutations, the gene is downregulated, leading to disruption in epidermal hydration and skin barrier dysfunction. In the immune-based model, T-helper 2 cells activate the type 2 immune response, increasing the production of cytokines (ie, interleukin [IL]-4, IL-13, and IL-31), which increase IgE synthesis and induce epidermal abnormalities. In addition, an overactivity of phosphodiesterase-4 contributes to the inflammatory response. We now recognize other important pathophysiologic components, such as an abnormal skin microbiome that is highly colonized by Staphylococcus aureus. The interplay between type 2 inflammation and S aureus is key.
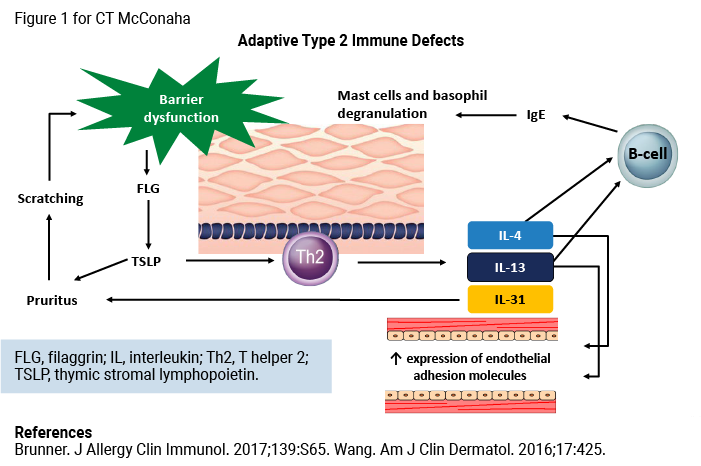
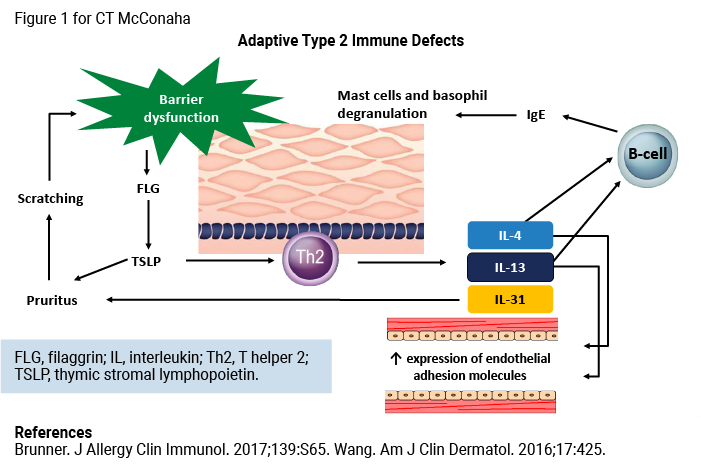
Understanding the pathophysiology of AD is important for pharmacists so that we can better appreciate the mechanisms of action of newer agents, how they treat both inflammation and symptoms— such as the itch we see commonly in AD—and how these agents will benefit patients.
Efficacy and Safety Considerations for New Biologic Agents
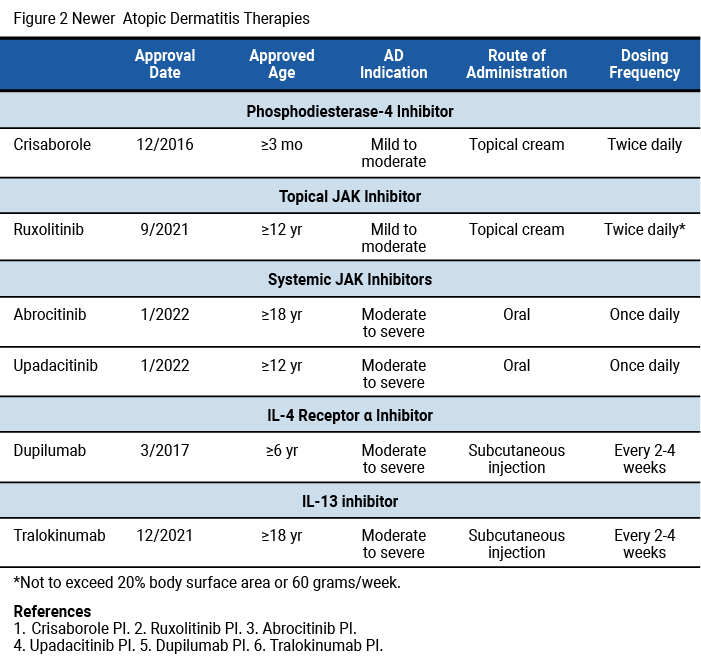
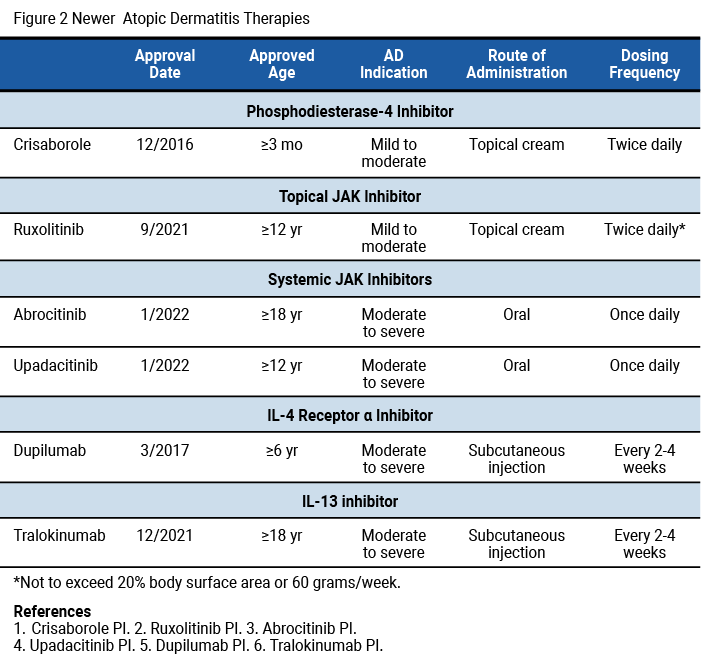
There are several new biologic medications for the pharmacist to be aware of (Figure 2), as well as several that are currently in phase III clinical trials and may come to market soon. When we are considering these new medications, specifically the JAK, IL-13, and IL-31 inhibitors, we must consider their risks and benefits. Throughout our presentation, we delved into clinical trials looking at the safety and efficacy of each agent. Although they are efficacious and add much-needed options for AD, we must consider adverse events and safety concerns and when they may or may not be appropriate to use in certain patients.
First, I think we must consider that uncontrolled AD has its own set of risks. For patients who develop AD at a younger age, long durations of uncontrolled AD can result in, for example, decreased sleep, missing school or work, skin infections, and hospitalization.
However, the risk of not adequately controlling AD must be weighed against the risks of using some of the newer agents. For example, in 2021, the FDA called for additional warning labels on the JAK inhibitors after a safety review showed that they were associated with an increased risk of cardiac events, serious infections, cancer, blood clots, or death.
Although not all JAK inhibitors have been studied in similar large safety clinical trials, the boxed warning was applied to the class as a whole and may affect the approval of pipeline agents coming to market. However, we do see many of these agents still playing a key role in patients with AD because of their efficacy and positive effect on quality of life. If patients do not have a cardiovascular risk, for example, these agents may be a great fit for their treatment plan.
Considerations for Shared Decision-Making and Accessibility When Choosing Therapies
An important role for pharmacists is talking with patients about the risk–benefit ratio of all the medications and helping them select the best treatment option. Several factors should be considered when selecting a treatment. We can look at clinical trial data for the efficacy of the medications, but just because the agent is the most efficacious does not mean it is the best one for a particular patient. We need to make very patient-specific recommendations and use the shared decision-making model when considering the best biologic treatment or any treatment for a patient with AD. We should consider the efficacy onset or how quickly the medication is going to work, as many patients have severe disease and are very uncomfortable, so they would prefer something that works quickly. In these cases, topical medication or phototherapy may not be the best choice. Other important considerations include the efficacy in terms of maximal effect that we can see from the agent, safety, and tolerability.
An important area where pharmacists help patients is with medication accessibility. When we think of cost, we should consider what is affordable for that particular patient, even if it is covered by their insurance plan. In addition, we should help educate and navigate patients through prior authorization processes when required and ensure that they have access to treatment while they await approval.
Finally, after we have addressed all of those points and selected the best medication for our patient, we need to remain vigilant and reassess regularly to see how the patient is responding to and tolerating therapy. Are they able to continue to afford the therapy? Has the clinical course of their disease state changed? Pharmacists need to continuously revisit these considerations to see if the therapy is appropriate for that patient to continue or when we might want to consider switching therapies.
Your Thoughts?
In your practice, what do you find are the most important considerations when helping patients with AD select the best treatment option? Answer the polling question and join the discussion by posting a comment.
Contact Clinical Care Options
For customer support please email: customersupport@cealliance.com
Mailing Address
Clinical Care Options, LLC
12001 Sunrise Valley Drive
Suite 300
Reston, VA 20191
You are now leaving the CCO site. The new destination site may have different terms of use and privacy policy.