Thank you for your interest in CCO content. As a guest, please complete the following information fields. These data help ensure our continued delivery of impactful education.
Become a member (or login)? Member benefits include accreditation certificates, downloadable slides, and decision support tools.

Clinical Assistant Professor
Department of Pharmacy Practice
College of Pharmacy
Clinical Pharmacist
Infectious Diseases
UI Health
Chicago, Illinois
Rodrigo Burgos, PharmD, MPH: consultant/advisor/speaker: Janssen Vaccines, Merck, Moderna, OptumRx, ViiV Healthcare.
Key Takeaways
The management of treatment-experienced people with HIV (PWH) is an evolving art and science. For antiretroviral therapy (ART) regimen options after failure of a first or second ART regimen, the Department of Health and Human Services (DHHS) guidelines provide useful recommendations based on the literature and expert opinions. However, for PWH with a history of multiple regimen failures, PWH with resistance to multiple drug classes, or heavily treatment‒experienced (HTE) PWH with drug resistance, the guidance is less specific and abundant. The treatment management for these individuals relies on healthcare professional experience, extrapolation from scientific literature, and an individualized treatment approach. Nevertheless, some basic principles can be applied in most of these complex cases.
Creating Salvage Regimens With ARTs With High Barrier to Resistance
For HTE PWH without virologic suppression, to avoid the development of additional resistance, DHHS recommends against simply adding a single active agent to supplement a failing regimen (what we veterans used to call regimen “intensification” or “intensifying”). Instead, they recommend a new regimen consisting of at least 2 fully active agents, at least 1 of which has a high genetic barrier to the development of HIV-1 resistance. As of the end of 2022, boosted darunavir, dolutegravir, and bictegravir were cited by DHHS as agents with high barriers to resistance.
Integrase Inhibitors for Resistant HIV
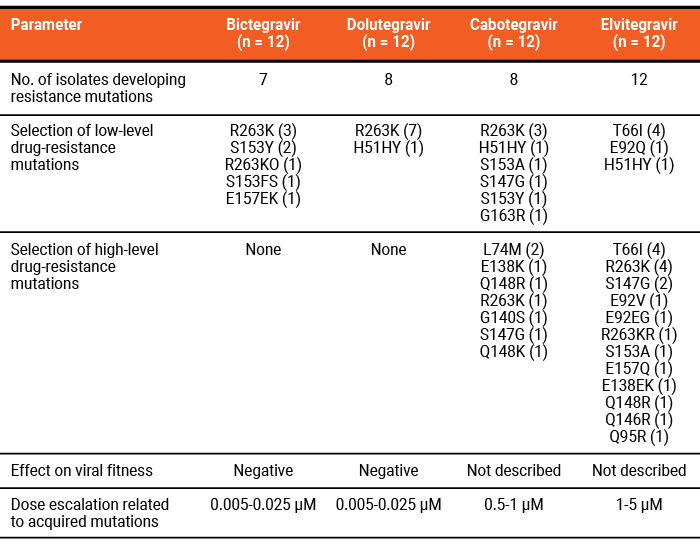
Although cabotegravir is newest to the market and has not yet accrued the body of data that older integrase strand transfer inhibitors (INSTIs) have, in vitro data suggest that its genetic barrier to resistance may be lower than dolutegravir or bictegravir but higher than raltegravir and elvitegravir. A small viral passage study in B and non-B HIV-1 subtype strains exposed to escalating concentrations of INSTIs found a lower selection of mutations, complex resistance patterns, and the need for dose escalation with dolutegravir and bictegravir compared with cabotegravir and elvitegravir (Table 1).
Whether this experimental finding translates to higher treatment-emergent resistance with cabotegravir remains to be seen with increased clinical implementation of this new drug. Early real-world data from 2 reports do not suggest high rates of treatment-emergent INSTI resistance in PWH receiving cabotegravir in Germany (2/200) or across 5 European countries (1/430). In the United States, a real-world cohort of patients receiving cabotegravir reported low rates of virologic failure, but data on emergence of INSTI resistance from cabotegravir use were not available. Despite limited data, so far cabotegravir appears to have a fairly high genetic barrier to resistance.
Table 1. In Vitro Viral Passage Study of B and Non-B Clades of HIV-1 in Escalating ART Concentrations

Individualizing Salvage Regimens
If no fully active drug with a high genetic barrier to resistance is available, DHHS recommends a regimen with 3 fully active agents (or partially active agents that add up to 3 fully active agents) for the treatment of HTE PWH without virologic control. One may consider traditional agents based on genotypic or phenotypic susceptibility, such as boosted protease inhibitors (PIs) and nucleos(t)ide reverse-transcriptase inhibitors (NRTIs).
When constructing a salvage regimen, the use of partially active agents can be challenging, particularly when estimating their residual activity. However, data from the EARNEST and NADIA studies demonstrated that NRTIs may retain long-term activity as part of a regimen even when genotypic susceptibility indicates otherwise. The EARNEST trial observed high rates (86%) of virologic suppression (<400 copies/mL) through 144 weeks in PWH receiving 2-3 NRTIs plus an older PI (lopinavir/ritonavir) who had varying degrees of genotypic NRTI resistance after failing first-line regimens consisting of 2 NRTIs plus a nonnucleoside reverse-transcriptase inhibitor (NNRTI).
Similarly, the NADIA trial observed high rates (>84%) of virologic suppression (<400 copies/mL) at Week 96 in PWH receiving either emtricitabine/tenofovir disoproxil fumarate or lamivudine/zidovudine in combination with either dolutegravir or darunavir/ritonavir who had baseline NRTI resistance after failing a regimen with 2 NRTIs plus an NNRTI.
Other fully active agents that may be considered when constructing a salvage regimen are older agents with unique mechanisms of action, such as enfuvirtide and maraviroc (for CCR5-tropic virus), or those with newer mechanisms of action, such as ibalizumab and fostemsavir.
A New Long-Acting Option for HTE PWH
On December 22, 2022, the FDA approved lenacapavir, an HIV-1 capsid inhibitor interfering with replication at multiple points in the viral life cycle. Lenacapavir can be used in adults with limited treatment options due to resistance, intolerance, or safety concerns, and it is dosed subcutaneously every 6 months. Similarly to when long-acting cabotegravir plus rilpivirine entered the market, the availability of a long-acting, new-in-class agent with semiannual administration has rejuvenated excitement for the future of HIV management with long-acting drugs. However, because lenacapavir is only part of an optimized, individualized ART regimen, its use will be limited to the smaller HTE population in which it was studied. Until data in larger patient populations (eg, treatment naive, first- or second-line treatment failures) demonstrate its role for more general use, I expect to see lenacapavir among other salvage agents used with optimized backgrounds (Table 2).
Table 2. ARTs With Novel Mechanisms for HTE PWH
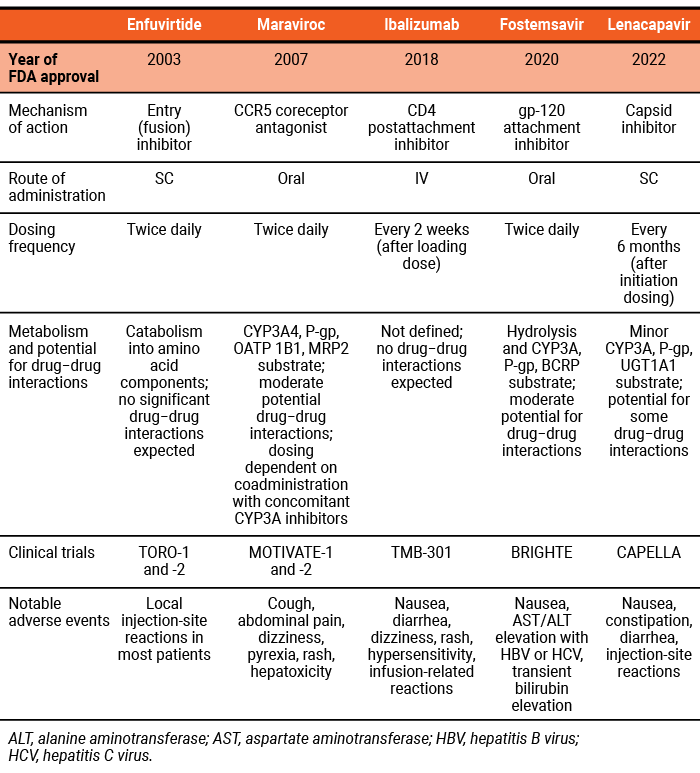

ALT, alanine aminotransferase; AST, aspartate aminotransferase; HBV, hepatitis B virus; HCV, hepatitis C virus.
Your Thoughts?
In your clinical practice, what ART regimens are you using for PWH who are HTE? Please join the discussion by leaving a comment.
Contact Clinical Care Options
For customer support please email: customersupport@cealliance.com
Mailing Address
Clinical Care Options, LLC
12001 Sunrise Valley Drive
Suite 300
Reston, VA 20191
You are now leaving the CCO site. The new destination site may have different terms of use and privacy policy.